
Dec. 15, 2023 – For much of his life, 32-year-old Michael Smith had a war going on in his head.
After a big meal, he knew he should be full. But an inexplicable hunger would drive him to pick up the fork again.
Cravings for fried chicken or gummy bears overwhelmed him, fueling late-night DoorDash orders that – despite their bounty of fat and sugar — never satisfied him.
He recalls waking up on the couch, half-eaten takeout in his lap, feeling sluggish and out of control.
“It was like I was food drunk,” recalls Smith, who lives in Boston. “I had a moment I looked at myself in the mirror. I was around 380 pounds, and I said, ‘OK, something has got to give.’”
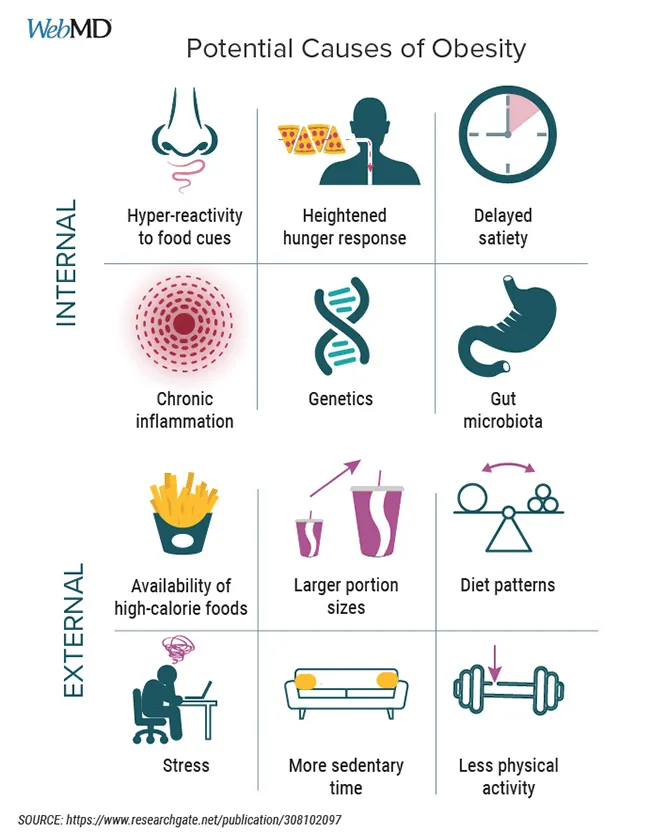
Smith is among the 42{44f8fb62c767d9a0e024bd2a609adf80ac0b081e02fd95d47dd066fb0a89173b} of U.S. adults living with obesity, a misunderstood and stubbornly hard-to-manage condition that doctors have only recently begun to call a disease. Its root causes have been debated for decades, with studies suggesting everything from genes to lifestyle to a shifting food supply loaded with carbohydrates and ultra-processed foods. Solutions have long targeted self-discipline and a simple “eat less, move more” strategy with remarkably grim results.
Those who successfully slim down tend to gain back 50{44f8fb62c767d9a0e024bd2a609adf80ac0b081e02fd95d47dd066fb0a89173b} of that weight within 2 years, and 80{44f8fb62c767d9a0e024bd2a609adf80ac0b081e02fd95d47dd066fb0a89173b} within 5 years. Meanwhile, the obesity epidemic marches on.
But a new frontier of brain-based therapies – from GLP-1 agonist drugs thought to act on reward and appetite centers to deep brain stimulation aimed at resetting neural circuits – has kindled hope among patients like Smith and the doctors who treat them. The treatments, and theories behind them, are not without controversy. They’re expensive, have side effects, and, critics contend, pull focus from diet and exercise.
Butmost agree that in the battle against obesity, one crucial organ has been overlooked.
“Obesity, in almost all circumstances, is most likely a disorder of the brain,” said Casey Halpern, MD, an associate professor of neurosurgery at the University of Pennsylvania. “What these individuals need is not simply more willpower, but the therapeutic equivalent of an electrician that can make right these connections inside their brain.”
A Break in the Machine
Throughout the day, the machine that is our brain is constantly humming in the background, taking in subtle signals from our gut, hormones, and environment to determine when we’re hungry, how food makes us feel, and whether we are taking in enough energy, or expending too much, to survive.
“We like to think that we have control over what we eat, but the brain is also integrating all of these factors that we don’t fully understand in ways that shape our decisions,” said Kevin Hall, PhD, an obesity researcher with the National Institute of Diabetes and Digestive and Kidney Diseases. “I liken it to holding your breath. I can do that for a period of time, and I have some conscious control. But eventually, physiology wins out.”
Mounting evidence suggests that in people with obesity, something in the machine is broken.
One seminal 2001 study in The Lancet suggested that, like people addicted to cocaine or alcohol, they lack receptors to the feel-good brain chemical dopamine and overeat in pursuit of the pleasure they lack.
A recent study, not yet published, from Hall’s lab drew a slightly different conclusion, suggesting that people with obesity actually have too much dopamine, filling up those receptors so the pleasure spike from eating doesn’t feel like much.
“It’s kind of like trying to shout in a noisy room. You’re going to have to shout louder to have the same effect,” said Hall.
Gut-brain pathways that tell us we’re full may also be impaired.
In another study, Yale researchers tube-fed 500 calories of sugar or fat directly into the stomachs of 28 lean people and 30 people with obesity. Then they observed brain activity using functional magnetic resonance imaging (fMRI).
In lean people, about 30 regions of the brain quieted after the meal, including parts of the striatum (associated with cravings).
In those with obesity, the brain barely responded at all.
“In my clinic, patients will often say ‘I just finished my dinner, but it doesn’t feel like it,’” said senior author Mireille Serlie, MD, PhD, an obesity researcher at the Yale School of Medicine. “It may be that this nutrient-sensing interaction between the gut and the brain is less pronounced or comes too late for them after the meal.”
Halpern recently identified a brain circuit linking a memory center (hippocampus) to an appetite control region (hypothalamus). In people with obesity and binge eating disorder, the circuit appears jammed. This may cause them to, in a sense, forget they just ate.
“Some of their eating episodes are almost dissociative – they’re not realizing how much they are eating and can’t keep track of it,” he said.
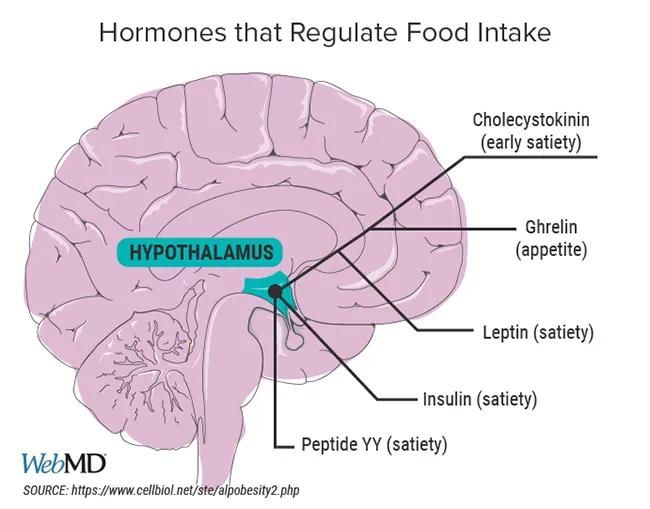
Another brain system works to maintain longer-term homeostasis – or weight stability. Like a set thermostat, it kicks on to trigger hunger and fatigue when it senses we’re low on fat.
The hormone leptin, found in fat cells, sends signals to the hypothalamus to let it know how much energy we have on board.
“If leptin levels go up, it signals the brain that you have too much fat and you should eat less to return to the starting point,” said Rockefeller University geneticist Jeffrey Friedman, MD, PhD, who discovered the hormone in 1994. “If you have too little fat and leptin is low, that will stimulate appetite to return you to the starting point.”
In people with obesity, he said, the thermostat – or set point the body seeks to maintain – is too high.
All this raises a crucial question: How do these circuits and pathways malfunction in the first place?
What Breaks the Brain?
Genes, scientists agree, play a role.
Studies show that genetics underlie as much as 75{44f8fb62c767d9a0e024bd2a609adf80ac0b081e02fd95d47dd066fb0a89173b} of people’s differences in body mass index (BMI), with certain gene combinations raising obesity risk in particular environments.
While hundreds of genes are believed to have a small effect, about a dozen single genes are thought to have a large effect. (Notably, most influence brain function.) For instance, about 6{44f8fb62c767d9a0e024bd2a609adf80ac0b081e02fd95d47dd066fb0a89173b} of people with severe obesity since childhood have mutations in a gene called MC4R (melanocortin 4 receptor), which influences leptin signaling.
Still, genetics alone cannot account for the explosion in obesity in the U.S. over the last 50 years, says epidemiologist Deirdre Tobias, ScD, an assistant professor of medicine at Harvard Medical School.
At the population level, “our genes don’t change that much in less than a generation,” she said.
But our food supply has.
Ultra-processed foods – those containing hydrogenated oils, high-fructose corn syrup, flavoring agents, emulsifiers, and other manufactured ingredients – now make up about 60{44f8fb62c767d9a0e024bd2a609adf80ac0b081e02fd95d47dd066fb0a89173b} of the food supply.
“The evidence is fairly consistent indicating that there’s something about these foods that is possibly causing obesity,” said Tobias.
In one telling 2019 study, Hall and his colleagues brought 20 men and women into a study center to live for a month and tightly controlled their food intake and activity. One group was provided with meals with 80{44f8fb62c767d9a0e024bd2a609adf80ac0b081e02fd95d47dd066fb0a89173b} of calories from ultra-processed food. The other was given meals with no processed food.
The three daily meals provided had the same calories, sugars, fats, fiber, and carbohydrates, and people were told to eat as much as they wanted.
Those on the ultra-processed diet ate about 500 calories more per day, ate faster, and gained weight. Those on the unprocessed diet lost weight.
“This is a stark example of how, when you can change the food environment, you cause really remarkable changes in food intake without people even being aware that they are overeating,” said Hall.
Just what it is about these relatively novel foods that may trigger overeating is unclear. It could be the crunch, the lack of water content, the engineered balance of sugar/salt/fat, their easy-to-devour texture, or something else.
Some research suggests that the foods may interfere with gut-brain signaling that tells the brain you’re full.
“Evidence is amassing that the nutritional content of processed foods is not accurately conveyed to the brain,” wrote Dana Small, PhD, a neuroscientist at Yale, in a recent perspective paper in Science.
Even more concerning: Some animal studies suggest processed foods reprogram the brain to dislike healthy foods.
And once these brain changes are made, they are hard to reverse.
“The problem is, our brain is not wired for this,” said Halpern. “We are not evolved to eat the food we are eating, so our brain adapts, but it adapts in a negative way that puts us at risk.”
That’s why changing the food environment via public policy must be part of the solution in combating obesity, Tobias said.
A New Era of Brain-Based Solutions
In the spring of 2021, after years of trying and failing to lose weight via the “move more, eat less” model, Michael Smith began to take a medication called Vyvanse. The drug was approved in 2008 for attention deficit hyperactivity disorder, but since it also influences levels of the hormones dopamine and norepinephrine to reduce cravings, it is now frequently prescribed for binge eating disorder.
“That was pretty much how I got rid of my first 60 to 70 pounds,” Smith said.
A few months later, after he hit a plateau, he had surgery to shrink the size of his stomach – a decision he now second-guesses.
While it kept him from overeating for a time, the fried chicken and gummy bear cravings returned a few months later.
His doctor, Fatima Cody Stanford, MD, put him on a second medication: semaglutide, or Wegovy, the weekly shot approved for weight loss in 2021. It works, in part, by mimicking glucagon-like peptide-1 (GLP-1), a key gut hormone that lets your brain know you are full.
The weight began to fall off again.
Smith’s success story is just one of many that Stanford, an obesity medicine doctor-scientist at Harvard, has heard in her office in recent years.
“I do not believe these drugs are a panacea,” she said. “There are non-responders, and those are the patients I take off the medication. But for the high-responders, and there are many of them, they are telling me, ‘Oh my gosh. For the first time in my life, I am not constantly thinking about eating. My life has changed.’”

A Multi-Pronged Approach
Halpern, at Penn, has also been hearing success stories.
In recent years, he has placed permanent electrodes in the brains of three people with grade III, or severe, obesity and binge eating disorder.
All had tried exercise, dieting, support groups, medication, and weight loss surgery to no avail.
The electrodes modulate an area in the center of the brain called the nucleus accumbens, which in mice studies has been shown to reduce cravings when stimulated.
Thus far, all three are seeing promising results.
“It’s not like I don’t think about food at all,” one of them, Robyn Baldwin, told The New York Times. “But I’m no longer a craving person.”
Halpern is now extending the trial to more patients and hopes to ultimately include other areas of the brain, including those that involve memory.
He imagines a day when people with severe obesity, who have failed conventional treatments, can walk into a clinic and have their brain circuits assessed to see which ones may be misfiring.
Many might find relief with noninvasive brain stimulation, like transcranial magnetic stimulation (already in use for depression). Others might need a more extreme approach, like the deep brain stimulation, or DBS, therapy Halpern used.
“Obviously, DBS is hard to scale, so it would have to be reserved for the most severe patients,” he said.
Still, not everyone believes brain-based drugs and surgeries are the answer.
David Ludwig, MD, PhD, a professor of nutrition at the Harvard School of Public Health, played a key role in the discovery of GLP-1 and acknowledges that “of course” the brain influences body composition. But to him, explaining obesity as a disease of the brain oversimplifies it, discounting metabolic factors such as a tendency to store too much fat.
He noted that it’s hard to get drug companies, or any agencies, to fund large clinical trials on simple things like low-carbohydrate diets or exercise programs.
“We need all the tools we can get in the battle against the obesity epidemic, and new technologies are worth exploring,” he said. “However, the success of these drugs should not lead us to deprioritize diet and lifestyle interventions.”
Stanford, who has received consulting fees from Wegovy, believes the future of treatment lies in a multi-pronged approach, with surgery, medication, and lifestyle changes coalescing in a lasting, but fragile, remission.
“Unfortunately, there is no cure for obesity,” said Stanford, whose patients often have setbacks and must try new strategies. “There are treatments that work for a while, but they are constantly pushing up against this origin in the brain.”
Smith says understanding this has been a big part of his success.
He is now a leaner and healthier 5-foot-6 and 204 pounds. In addition to taking his medication, he walks to work, goes to the gym twice a week, limits his portions, and tries to reframe the way he thinks about food, viewing it as fuel rather than an indulgence.
Sometimes, when he looks in the mirror, he is reminded of his 380-pound self, and it scares him. He doesn’t want to go back there. He’s confident now that he won’t have to.
“There is this misconception out there that you just need to put the fork down, but I’m learning it’s more complicated than that,” he said. “I intend to treat this as the illness that it is and do what I need to combat it so I’m able to keep this new reality I have built for myself.”


